
Can understanding the anatomy and function of the long thoracic nerve help individuals make informed healthcare decisions after an injury to the nerve?
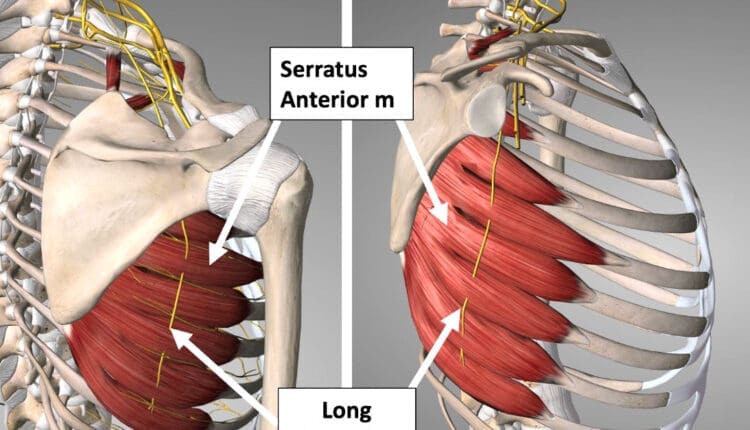
Table of Contents
Long Thoracic Nerve
Also referred to as the posterior thoracic nerve, the long thoracic nerve/LTN is a thin superficial nerve that runs from the cervical spine to the chest wall side of the trunk. It supplies motor function to the thorax’s serratus anterior muscle, helping stabilize the shoulder blade. Injury to this nerve can cause limited or abnormal shoulder and shoulder blade motion, including difficulty raising the arm during overhead reaching.
Anatomy
The long thoracic nerve originates from the ventral rami of cervical nerves C5, C6, and C7. (Waxenbaum JA, Reddy V, Bordoni B. 2023) In some individuals, the root from C7 is absent; in others, a small nerve root branches from C8. The nerve roots from C5 and C6 go through the medial scalene muscle to join the C7 nerve. It travels behind the brachial plexus axillary artery and vein and courses down the lateral side of the thorax. The long thoracic nerve terminates at the lower portion of the serratus anterior muscle, sending small nerve tendrils to each muscle’s projections, which attach to the ribs. Because the long thoracic nerve is located on the lateral side of the chest, it is vulnerable to injury during sports or surgical procedures. The nerve also has a smaller diameter than other cervical and brachial plexus nerves, which increases its potential for injury.
Function
The long thoracic nerve attaches to the underside of the shoulder blade and inserts as muscular slips into the ribs. It supplies motor function to the serratus anterior muscle, essential for normal shoulder motion. When it contracts, it pulls the shoulder blade against the ribs and thorax, helping to move and stabilize the arm as it moves forward and up during shoulder motions. Injury to the long thoracic nerve causes a condition called scapular winging. This occurs when the serratus anterior muscle becomes weakened or paralyzed after injury. (Lung K, St Lucia K, Lui F. 2024)
Susceptibility to Injury
The LTN is relatively unprotected and can be damaged by several things, including:
- Heavy backpacks
- Sports
- Activities the body is not used to, like digging
- Using crutches
Conditions
Injury to the long thoracic nerve may occur as a result of trauma, lifting heavy weights above the shoulder, or a surgical procedure. Surgical procedures that may place the nerve at risk for injury may include: (Lung K, St Lucia K, Lui F. 2024)
- Axillary lymph node dissection
- Improperly placed intercostal drains
- Chest tube placements
- Mastectomy
- Thoracotomy
The long thoracic nerve is protected during these procedures by the surgeon and proper surgical technique, but occasionally, difficulties arise during surgery, and the nerve may become injured. Individuals may also have an anatomical variance that places their nerves in varying positions. The surgeon may not see it and accidentally injure their nerves during surgery.
The superficial long thoracic nerve may also be injured during sports or trauma to the trunk. A blow to the side or a sudden overhead stretch to the shoulder may be enough to damage the nerve, paralyzing the serratus anterior muscle.
Weakness or paralysis of the serratus anterior muscle will result in a winged scapula. To test for this:
- Stand about two feet from a wall, facing it.
- Place both hands on the wall and gently push against it.
- If one of the shoulder blades sticks out abnormally, it could be a winged scapula.
- Have a family member or friend stand behind you and check the shoulder blade position.
- If you suspect a winged scapula, visit a physician who can assess the condition and determine if there is a long thoracic nerve injury.
Winging the scapula may result in difficulty lifting the arm overhead. The serratus anterior muscle works with other scapular stabilizers, such as the upper trapezius and levator scapula, to properly position the shoulder blade when lifting the arm. Failure of the serratus to stabilize the shoulder blade may make lifting the arm impossible.
Clinical examination is usually used to diagnose a long thoracic nerve injury. X-rays and MRIs cannot show the nerve injury directly, although an MRI can show some secondary signs to help confirm the diagnosis. An electromyographic or EMG test may also be performed to examine the function of the long thoracic nerve.
Treatment and Rehabilitation
Treatment for LTN pain and reduced movement may include:
- Rest
- Heat or ice
- Anti-inflammatory pain medication
- Neck support or a pillow
- Avoiding strenuous activity and driving
If the long thoracic nerve is severely injured and the serratus anterior is completely paralyzed, the best course of action is to be active and monitor the condition. Full recovery of arm function can take one to two years. If permanent nerve injury has occurred, surgery may be an option to restore shoulder motion and function. Several different kinds of surgery can be used to address winged scapula. (Vetter M. et al., 2017)
- One involves transferring the pectoralis major tendon to the scapula (Vetter M. et al., 2017) so it functions as the serratus.
- Often, the tendon has to be lengthened, which may be done using part of the hamstring tendon.
- After surgery, individuals will likely wear a sling on their arm for a few weeks, and then gentle range-of-motion exercises will be initiated.
- After eight to ten weeks, gentle progressive strengthening of the new tendon can begin.
- Full shoulder motion and strength recovery are expected six to 12 months after surgery.
Physical therapy may be used to help improve serratus anterior functions. (Berthold J. B., Burg T. M., & Nussbaum R. P. 2017) Exercises to strengthen serratus function may include:
Supine Punches
- Lie on your back and raise both arms toward the ceiling.
- Make a fist and punch up toward the ceiling.
- Ensure the motion is steady and deliberate, and keep the elbow straight.
- Hold the position for three seconds, then slowly lower the arm to the starting position.
- Perform 10 to 15 repetitions.
- Holding a small dumbbell in your hands can make the exercise more challenging.
Pushup
- Lie on your stomach and place your hands flat on the ground by your shoulders as if you were going to perform a pushup.
- Perform a pushup and press further, allowing the shoulder blades to wrap around the thorax.
- Hold this position for three seconds, and slowly release.
- Perform 10 to 15 reps.
- If this is too difficult, perform the pushup against a wall to reduce the effect of gravity on the exercise.
Scapular Winging in Depth
References
Waxenbaum, J. A., Reddy, V., & Bordoni, B. (2024). Anatomy, Head and Neck: Cervical Nerves. In StatPearls. www.ncbi.nlm.nih.gov/pubmed/30844163
Lung, K., St Lucia, K., & Lui, F. (2024). Anatomy, Thorax, Serratus Anterior Muscles. In StatPearls. www.ncbi.nlm.nih.gov/pubmed/30285352
Vetter, M., Charran, O., Yilmaz, E., Edwards, B., Muhleman, M. A., Oskouian, R. J., Tubbs, R. S., & Loukas, M. (2017). Winged Scapula: A Comprehensive Review of Surgical Treatment. Cureus, 9(12), e1923. doi.org/10.7759/cureus.1923
Berthold, J. B., Burg, T. M., & Nussbaum, R. P. (2017). Long Thoracic Nerve Injury Caused by Overhead Weight Lifting Leading to Scapular Dyskinesis and Medial Scapular Winging. The Journal of the American Osteopathic Association, 117(2), 133–137. doi.org/10.7556/jaoa.2017.025
Disclaimers
Professional Scope of Practice *
The information herein on "Exploring the Long Thoracic Nerve: Anatomy and Injury" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's wellness blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-C) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on dralexjimenez.com, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and directly or indirectly support our clinical scope of practice.*
Our office has reasonably attempted to provide supportive citations and has identified the relevant research studies or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card




